

Abstract
Background
Fanconi anemia (FA) is a condition characterized by congenital malformations, low height, and progressive bone marrow failure during childhood, genomic instability and hypersensitivity to DNA cross-linking agents. Bone marrow transplantation (BMT), is currently the only treatment capable to restore normal hematopoiesis and improve survival of these patients. To achieve a successful allogeneic BMT, a normal T-cell immunity reconstitution is required.1,2
Objective
To describe the kinetics of immune reconstitution in six patients with FA after BMT, having used a reduce intensity conditioning regimen, well as associated infections during the post-transplant process.
Methods
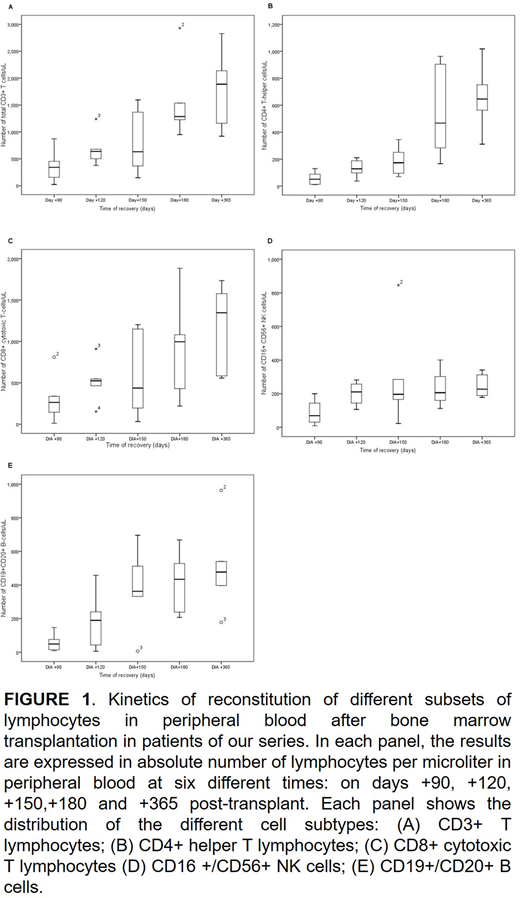
We describe the distribution in peripheral blood of CD3+ T lymphocytes, CD16 +/CD56+ NK cells, CD4+ helper T lymphocytes, CD8+ cytotoxic T lymphocytes and CD19+/CD20+ B cells, in six patients with FA, after BMT from an HLA-matching sibling and complete chimerism, on days +90, +120, +150, +180, +210 and +360. The conditioning regimen employed consisted of fludarabine (Flu) 150 mg/m2, cyclophosphamide 20 mg/kg and rabbit anti-thymocyte globulin (r-ATG) 20 mg/kg. Infection was determined by a positive reaction of the DNA polymerase chain to Cytomegalovirus (CMV), Epstein-Barr virus, Adenovirus and BK virus (BKV), as well as galactomannan antigen and antibodies against Candida sp, or positive bacterial cultures.
Results
We observed different kinetics regarding the recovery of different lymphocyte subpopulations, starting from day +90. CD16+/CD56+ NK cells recovered first, between days 90 and 120, followed by CD8+ T lymphocytes between day +120 and +150, CD19+/CD20+ B cells between day +180 and +210, and finally, CD4+ T lymphocytes starting from day 210. Five patients presented infection in the post-BMT stage. Four patients before +90, developed CMV infection, based on positive reaction of the CMV polymerase chain. All patient responses to ganciclovir therapy and no CMV disease were documented. The fifth patient presented with meningitis due to Lysteria monocitogenes and BKV hemorrhagic cystitis at day +153; this patient had the diagnosis of chronic-graft versus host disase, and was treated with ampicillin, rifampicin and intravenous immunoglobulin, evolving satisfactorily. All patients remain alive and well.
Discussion
Most patients in our report developed CMV infection, as being reported with FLU and anti-thymocyte globulin combination. We observed a later reconstitution in comparison with patients in whom lower doses of r-ATG (<10 mg/kg) have been used3. In our group of patients, reconstitution of NK cells and CD8+ T lymphocytes, helped to reduce the frequency of asymptomatic viral infections, as reconstitution of innate immunity and cytotoxic CD8+ T lymphocytes can achieve effective antiviral effector responses, allowing for the control of viral infections, until reconstitution of CD4+ T lymphocytes were fully achieved. The infectious complications associated with this prolonged state of profound immunosuppression and late immune reconstitution, can be attenuated with a closely follow-up for these infectious agents through PCR-mediated detection techniques, which allows an early diagnosis and prompt treatment.
Conclusion
Immunological reconstitution after a BMT in FA patients is determinant for morbidity and mortality, mainly due to opportunistic infections and GVHD. We observed that recovery kinetics of different lymphocyte populations is different in cases in which higher doses of r-GAT are used, also an early detection and prompt treatment of opportunistic infections may be determinant for patient's survival.
Conflict-of-interest disclosure: The authors declare they have nothing to disclose.
Correspondence: Gerardo López-Hernández. loherge@gmail.com
Bibliography
Ogonek J, Kralj Juric M, Ghimire S, Varanasi PR, Holler E, Greinix H, et al. Immune reconstitution after allogenic hematopoietic stem cell transplantation. Front immunol. 2016; 7 (507):1-15.
Smith AR, Wagner JE. Current clinical management of Fanconi anemia. Expert Rev Hematol. 2012; 5 (5): 513-522.
Perlingeiro-Beltrame M, Malvezzi M, Bonfim C, Tadeu Covas D, Pasquini R. Immune reconstitution in patients with Fanconi anemia after allogeneic bone marrow transplantation. Cytotherapy. 2014; 0: 1e14.
No relevant conflicts of interest to declare.

